Differential diagnosis of acute cholecystitis
Perforated peptic ulcer. For this disease the Mondor’s triad (“knife-like” pain, tension of muscles of front abdominal wall and ulcerous anamnesis) and positive Spizharny’s sign are characteristic (disappearance of hepatic dullness). On the abdominal X-ray gram under the right copula of diaphragm free gaze can be found.
Right-side kidney colic. Pain at right-side kidney colic also can be localized in right hypochondrium. However, it is always accompanied by disorders of urination. Kidney pain often irradiates downward along passing of ureter. For this pathology micro- or macrohaematuria, presence of renal concrements exposed at sonography and on the urograms. Absence of renal function during chromocystoscopy can be characteristic.
Acute appendicitis. It is needed always to remember, that the subhepatic location of the pathologically changed appendix is also able to show up pain in right hypochondrium. However, for patients with acute appendicitis beginning of pain in epigastric region, absence of hepatic anamnesis, expressed dyspeptic phenomena, inflammatory changes from the side of gallbladder at sonography are inherent.
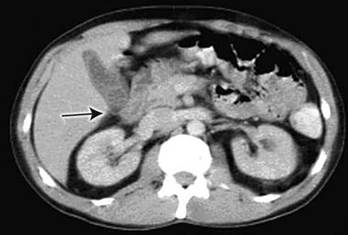
Figure 9 – Computed tomography on admission showed pericholecystic inflammation, suggesting acute cholecystitis, and a possible gallstone

Figure 10 – Endoscopic retrograde cholangiopancreatography
Heart attack, myocardial infarction. The so called cholecystocardial syndrome which often imitates stenocardia pain, suspicion of heart attack or myocardial infarction can develop. Electrocardiography examination is decisive in establishment of diagnosis. However, laparoscopy is applied in doubtful cases.
Acute pancreatitis. Acute pancreatitis is accompanied by the expressed upper abdominal pain. During palpation in left costovertebral corner patients feel painfulness (Mayo-Robson’s sign).
Дата добавления: 2015-07-04; просмотров: 1388;