Clinical diagnostics of acute appendicitis
The disease begins with a sudden pain in the abdomen. It is localized in a right iliac region, has moderate intensity, constant character and not irradiate. With 70% of patients the pain arises in epigastric region or other part of abdominal cavity – it is an “epigastric phase” of acute appendicitis. In 2–4 hours it moves to the place of appendix existence (Kocher’s sign). At coughing patients mark strengthening of pain in a right iliac region – it is a positive cough symptom.
Together with it, nausea and vomiting that have reflex character can disturb a patient. The temperature of body of most patients rises, but it is a low grade fever. The general condition of patients is usually normal and gets worse only in case of growth of destructive changes in appendix.
Painfulness is the basic and decisive signs of acute appendicitis during the examination by palpation in a right iliac region. Tension of muscle of abdominal wall is a positive symptom of peritoneum irritation.
Blumberg’s sign. After gradual pressing by fingers on a front abdominal wall from the place of pain quickly, but not acutely, the hand is taken away. Strengthening of pain is considered as a positive symptom in that place. Obligatory here is tension of muscles of front abdominal wall.
Voskresensky’s sign. By a left hand the shirt of patient is drawn downward and fixed on pubis. By the taps of 2–4 fingers of right hand epigastric region is pressed and during exhalation of patient quickly and evenly the hand slides in the direction of right iliac region, without taking the hand away. Thus there is an acute strengthening of pain.
Rovsign’s sign (fig. 1). By a left hand a sigmoid bowel is pressed to the back wall of stomach. By a right hand by balloting palpation a descending bowel is pressed. Appearance of pain in a right iliac region is considered as a sign characteristic of appendicitis.
Sitkovsky’s sign (fig. 2). A patient, that lies on left, feels the pain which arises or increases in the right iliac region. The mechanism of intensification of pain is explained by displacement of blind gut to the left, by drawing of mesentery of the inflamed appendix.
The Obrazcov’s sign (fig. 3). With the position of patient on the back by index and middle fingers the right iliac region of most painful place is pressed and the patient is asked to heave up the straightened right leg. At appendicitis pain increases acutely.
Bartomier’s sign (fig. 4) is the increase of pain intensity during the palpation in right iliac region of patient in position on the left side. At such pose an omentum and loops of small intestine is displaced to the left, and an appendix becomes accessible for palpation.
Rozdolsky’s sign. At percussion there is painfulness in a right iliac region.
The psoas (Roup’s) sign. This test is performed by having the patient lie on his left side. The examiner men slowly extends the patient’s right thigh, thus stretching the ileopsoas muscle. This will produce pain to make the sign positive. This indicates presence of irritative inflamed appendix in close proximity to the psoas muscle. This is possible in retrocaecal appendicitis.
Acute appendicitis in children. With children of infancy acute appendicitis can be seen infrequently, but, quite often

Figure 1 – Detection of Rovsign’s sign

Figure 2 – Detection of Sitkovsky’s sign
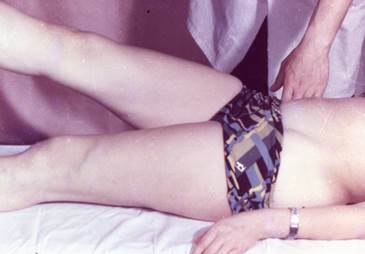
Figure 3 – Detection of Obrazcov’ssign

Figure 4 – Detection of Bartomier’s sign
carries atypical character. All this is conditioned, mainly, by the features of anatomy of appendix, insufficient of plastic properties of the peritoneum, short omentum and high reactivity of child’s organism. The inflammatory process in the appendix of children quickly makes progress and during the first half of days from the beginning of disease there can appear its destruction, even perforation. The child, more frequent than an adult, suffers vomiting. Its general condition gets worse quickly, and already the positive symptoms of irritation of peritoneum can show up during the first hours of a disease. The temperature reaction is also expressed considerably acuter. In the blood test there is high leukocytosis.
Acute appendicitis of the people of declining and old ages can be met not so often, as of the persons of middle ages and youth. This contingent of patients is hospitalized to hospital rather late: in 2–3 days from the beginning of a disease. Because of the promoted threshold of pain sensitiveness, the intensity of pain in such patients is small, therefore they almost do not fix attention on the epigastric phase of appendicitis. More frequent are nausea and vomiting, and the temperature reaction is expressed poorly. Tension of muscles of abdominal wall is absent or insignificant through old-age relaxation of muscles. But the symptoms of irritation of peritoneum keep the diagnostic value with this group of patients. Thus, the sclerosis of vessels of appendix results in its rapid numbness, initially gangrenous appendicitis develops. Because of such reasons the destructive forms of appendicitis prevail, often there is appendicular infiltrate.
With pregnant women both the bend of appendix and violation of its blood flow are causes of the origin of appendicitis. Increased in sizes uterus causes such changes. It, especially in the second half of pregnancy, displaces a blind gut together with an appendix upwards, and an overdistension abdominal wall does not create adequate tension. Together with that, psoas sign and Kocher’s sign, Bartomier’s sign have a diagnostic value at pregnant women.
Appendicitis at retrocecal and retroperitoneal location. Thus an appendix can be placed both in a free abdominal cavity and retroperitoneal. An atypical clinic arises, as a rule, at the retroperitoneal location. The patients complain of pain in lumbus or above the wing of right ileum. There they mark painfulness during palpation. Sometimes the pain irradiates to the pelvis and in the right thigh. The positive Rozanov’s sign – painfulness during palpation in the right Pti triangle is characteristic. In transition of inflammatory process on an ureter and kidney in the urines analysis red corpuscles can be found.
The pelvic location of appendix. In such patients the pain is localized above the right Poupart’s ligament and above pubis. At the very low placing of appendix at the beginning of disease the reaction of muscles of front abdominal wall on an inflammatory process can be absent. With transition of inflammation of an urinary bladder or rectum either the dysuria signs or diarrhaea develop. Distribution of process on internal genital organs provokes signs characteristic of their inflammation.
Appendicitis at the medial placing of appendix. The appendix in patients with such pathology is located between the loops of intestine, which is the large field of irritation of peritoneum. At these anatomic features mesentery is pulled in the inflammatory process, acute dynamic of the intestinal obstruction develops in such patients. The pain in the abdomen is intensive, widespread, the expressed tension of muscles of abdominal wall develops.
For the subhepatic location of appendix the pain is characteristic in right hypochondrium. During palpation painfulness and tension of muscles can be marked.
Left-side appendicitis appears infrequently and, as a rule, in case of the reverse placing of all organs; however it can occur at a mobile blind gut. In this situation all signs which characterize acute appendicitis will be exposed not on the right, as usually, but on the left.
Дата добавления: 2015-07-04; просмотров: 2729;