Hyper- and hypoglycemia
Under some conditions increase of glucose in blood can be observed. It is called hyperglycemia,and lowering the concentration of glucose is called hypoglycemia.
Changes of glucose levels over time in blood are investigated for the diagnosis of hyperglycemia, usually after taking 50 grams or 100 grams of glucose dissolved in warm water. It is the so-called sugar load – glucose tolerance test. Blood and urine samples are collected every 30 minute. When assessing the glycemic curves we pay attention to the time of maximum lifting, height of the rise and time for the glucose concentration to return to the original level.
|
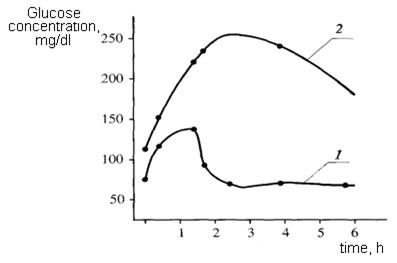
| Fig. 22. Glycemic curve in norm (1) and diabetes (2) |
In a healthy person after taking the glucose its amount in the blood is increased, reaching the peak after 30-45 minutes. Then its concentration in the blood begins to decrease and after 2 hours reduces to normal, but after 3 hours it is even slightly below normal (Fig. 22).
There is a number of indicators to evaluate the glycemic curves, the most important factor of which is a coefficient of Baudouin:
[(В-А)/А]х100, %,
where A – is the level of glucose in blood in an empty stomach; B – is the maximum glucose in blood after glucose load. Normally, this ratio seems to be about 50%. Values exceeding 80% indicate a serious disorder of carbohydrate metabolism.
Hormonal hyperglycemia occurs in any disturbance of the function of endocrine glands, hormones of which are involved in the regulation of carbohydrate metabolism.
One of the hyperglycemia’s reasons is diabetes mellitus.
Type 1 diabetes (insulin-dependent diabetes mellitus, IDDM) is associated with decreased formation of insulin. Usually it begins in childhood (12-15 years of age) as a consequence of autoimmune destruction of β-cells in the islets of the pancreas.
Type 2 diabetes begins in adulthood, develops gradually. Mechanisms of insulin signal transduction are damaged; the concentration of insulin in the blood may be normal or even elevated (insulin-independent diabetes mellitus, NIDDM). Receptors of target cells lose the ability to connect with a molecule of insulin.
Carbohydrate metabolism in diabetes mellitus is characterized by:
1. Glucokinase and glycogen syntase synthesis is sharply reduced, resulting in a sharp slowdown in the synthesis of glycogen.
2. Activity of glucose-6-phosphatase increases sharply, so the glucose-6-phosphate is dephosphorylated and enters the blood in the form of glucose.
3. Transport of glucose across cell membranes is reduced.
4. Gluconeogenesis is accelerated because insulin suppresses the activity of pyruvate carboxylase and glucose-6-phosphatase.
Thus, excess production and lack of use of glucose tissue occur in diabetes mellitus, causing hyperglycemia. Glucose in blood in severe forms can be up to 4-5 g/l and above. A body's homeostatic mechanism, when operating normally, restores the blood sugar level to a narrow range of about 4.4 to 6.1 mmole/l (0,82 to 1,10 g/l). The osmotic pressure of the blood is increased, which leads to dehydration of body cells. In connection with dehydration functions of the central nervous system are disturbed (hyperosmolar coma).
Glycemic curve (Glycemic index graph) in diabetes compared with that in healthy people is considerably stretched in time (Fig. 22).
Hyperglycemia is also being developed with an increase in production of glucagon - the hormone of α-cells of islets of Langerhans of the pancreas, which activates phosphorylase of the liver and promotes glycogenolysis. Similar action is typical of adrenaline.
An excess of glucocorticoids leads to hyperglycemia (which stimulates gluconeogenesis and inhibits hexokinase) and pituitary growth hormone (inhibits the synthesis of glycogen, promotes the formation of an inhibitor of hexokinase).
Hyperglycemia sometimes occurs during pregnancy, organic lesions of the central nervous system, liver disease of inflammation or degenerative nature.
Hypoglycemia is associated with a decrease in function of those endocrine glands, increasedfunctions of which lead to hyperglycemia. Hypoglycemia can be observed at Addison's disease (Addison’s disease is a chronic endocrine disorder - adrenal insufficiency, hypocortisolism, and hypoadrenalism), hypothyroidism, adenoma of the pancreas due to increased production of insulin. Hypoglycemia can be caused by starvation, prolonged physical work, taking β-ganglioplegics, sometimes it is observed during pregnancy and lactation. Hypoglycemia may occur when high doses of insulin are administered to patients with diabetes mellitus.
Glycosuria
Glycosuria is the result of altered carbohydrate metabolism as a result of pathological changes in the pancreas (diabetes mellitus, acute pancreatitis, etc.).
In severe forms of diabetes glucose in the urine can reach 8-10%. The osmotic pressure of urine is increased. The daily diuresis rises to 5-10 liters or more (polyuria). Dehydration develops as a consequence of it and increased thirst develops (polydipsia).
Less frequent glucosuria of renal origin, associated with failure of resorption of glucose in the kidney tubules.
Glycosuria may occur as a temporary phenomenon in some acute infectious and nervous diseases, after epilepsy, concussion.
Poisonings by morphine, strychnine, chloroform, phosphorus, are usually accompanied by glucosuria.
Glycosuria may be of nutritional origin, pregnancy glucosuria, and glucosuria with nervous stress states (emotional glycosuria).
Fructosuria iscongenital deficiency of the enzyme fructokinase (fructose-1-phosphate is not formed). The accumulation of fructose in blood leads to fructosuria.
Galactosemia. The reason is lack of the enzyme hexose-1-phosphaturidil transferase. It is characterized by accumulation of galactose and galactose-1-phosphate in the blood, vental retardation, cataracts of the lens.
Quiz Questions
1. List the major food sources of carbohydrates. What is the daily requirement for carbohydrates in the adult?
2. Describe the process of digestion and absorption of carbohydrates in the digestive tract.
3. Give the scheme glycogen synthesis from glucose, list the enzymes involved in this process.
4. Consider the mechanism of phosphorolytic cleavage of glycogen. What is the role of glycogen in the maintenance of glucose homeostasis?
5. What are the basic steps of glycolysis? What are the similarities and differences between aerobic and anaerobic glycolysis?
6. What is the energy value of breakdown of glucose under aerobic conditions?
7. What reaction includes measles cycle? What is its biochemical function?
8. What are the similarities and differences between glycolysis and fermentation?
9. What is meant by gluconeogenesis? What are the main stages of this process?
10. How does the glycerol phosphate shuttle mechanism and malate-aspartate shuttle system?
11. What is special about the exchange of fructose and galactose?
12. What are the hormones involved in regulating glucose homeostasis?
13. What is the chemistry of the pentose phosphate pathway of glucose metabolism?
14. What is the biological role of forming reduced forms of NADP?
15. List the disorders of carbohydrate metabolism that are known to you.
16. In what may be the cause of hyperglycemia and hypoglycemia?
Дата добавления: 2018-09-24; просмотров: 426;